 The UK coalition government has recently put forward proposals to further regulate migrants’ access to health care provision by extending charging for some services, for some groups. This includes an ‘immigration health surcharge’ (proposed around £150 - £200) as part of the Immigration Bill now slowly passing through Parliament, which would be imposed on all new ‘temporary’ entrants to the UK including workers on the points-based-system and their dependants, family members joining British citizens or permanent residents, and international students.
The UK coalition government has recently put forward proposals to further regulate migrants’ access to health care provision by extending charging for some services, for some groups. This includes an ‘immigration health surcharge’ (proposed around £150 - £200) as part of the Immigration Bill now slowly passing through Parliament, which would be imposed on all new ‘temporary’ entrants to the UK including workers on the points-based-system and their dependants, family members joining British citizens or permanent residents, and international students.
There is thus a fundamental shift from the rather fuzzy ‘ordinary resident’ requirement so far applied to most longer stay migrants who are legally resident in the UK, to permanent residence as the only valid basis of free access to the National Health Service. At the same time, there will eventually even be an erosion of the limited rights of some undocumented migrants - including UK-born children of undocumented parents - to some services, such as free access to Accident and Emergency hospital services, that have so far been granted on humanitarian and public health protection grounds.
These new measures to curtail rights of migrants to good health on the grounds of protecting public finances from ‘health tourism’, is a form of border control; that is, using affordability of health care as a way of regulating who is allowed into the country, and making it difficult for those seen as ‘undeserving’, often the most vulnerable of migrants, to remain. It is an instance of what Bosniak has written about as both ‘the question of access to territory’, and ‘the internal operation of the border’ where the border follows the immigrant inside the geographical national territory and impacts on their entitlement to, or restriction of, rights there based on status considerations.
Examples from history
It is the former, that is the role of health in determining who was allowed to cross the outside border into national territorial space that has been the focus of many medical history accounts. Ostensibly, the rationale of inclusion and exclusion of migrants in the past has been based more on public health than public financial concerns in receiving countries. However, historians have revealed a more complex picture. Markel and Stern have shown how the language and practice of public health as demonstrated in medical inspection processes at different ports and borders in the United States in the late 19th and early 20th centuries, reflected the assimilability of migrant groups according to factors such as skin colour, nationality, class, and relationship to labour market demand.
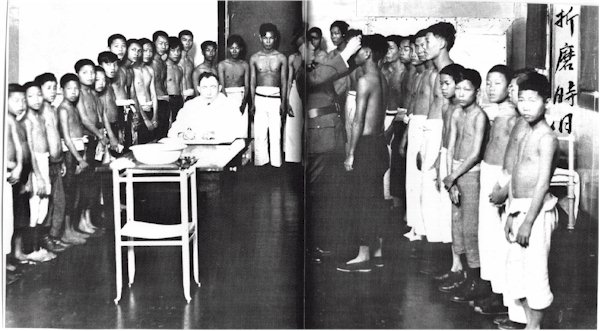
Physical Exams at Angel Island. Source: National Archives
For example, on Ellis Island in New York harbour where most of the migrants were from Europe, while the more impoverished steerage passengers underwent more stringent inspection than did first and second class passengers, concern around contagion, even for the former, was replaced eventually by scrutiny for chronic physical debilitation as expressed in terms like ‘poor physique’ and ‘feeble mindedness’. Even so, relatively few migrants were excluded for medical reasons alone. This was in contrast with medical inspections of largely Asian (particularly Chinese) migrants on Angel Island off the coast of San Francisco, who were much more likely to be treated with suspicion and hostility arising from racial and cultural prejudice, and subject to much more undignified processes of inspection for infection and a greater degree of rejection.
Similarly, Welshman and Bashford have analysed the historical Australian model of pre-entry medical screening particularly for communicable diseases like Tuberculosis, which is also the main basis of immigration control in Australia today. They state that in a country built on immigration, there was an explicit connection between race, imported disease seen to impact on public health, and migration law and policy, reflected for example in the Chinese Exclusion Act and the White Australia Policy in the early 20th century.
Global patterns in present day role of health in border control
It is clear that globally health plays a large part in emigration as well as immigration policies of nations today; for instance in determining who is allowed to leave one country to work in another country. There are examples in the stringent pre-departure medical testing requirements and regulation applying to diverse categories of workers migrating from lower income to higher income countries within the Asian region. Some of these health requirements and procedures operate within gender and class inequalities and have a detrimental impact on the sense of control poorer migrants have over decisions relating to their bodies.
Lindquist documents the lengths to which sponsors and labour recruitment agencies in the Indonesian island of Lombok go to prevent female domestic workers migrating to Malaysia or Singapore from becoming pregnant during the pre-departure phase such as not allowing them to visit their families, in order to protect the fees paid to the agencies by receiving country labour agencies. There is evidence from Sri Lanka that at least in the recent past, as part of pre-selection compulsory medical testing procedures instigated by receiving countries in the Gulf, women domestic workers were given contraceptive injections without a process of informed consent.
Overall, the historical as well as present day evidence that exists regarding the part played by health in border control suggests that, where they play a part in migration polices, they are less driven by straight-forward public health concerns. These health related policies and practices arising from them appear to exist firmly within a global framework of inequalities that continue to have a negative impact on disempowered and vulnerable migrants.